Raise The Alarm: How Well Do Emergency Rooms Serve Older Adults?
April 1, 2026

It’s perhaps one of our worst nightmares. A phone call during the night about a loved one needing to go to the local emergency room, due to a fall, a sharp pain, or some other type of serious problem. Or, you yourself suddenly feel dizzy or short of breath or in terrible pain that is not going away, and you are advised to head to an ER. No one wants to go to the hospital if they don’t have to, especially in today’s health care environment. Anyone who has watched at least one episode of The Pitt understands that hospital emergency departments are chaotic, crowded environments, often short of staff and definitely short of privacy and personal attention, hardly conducive to the kind of thoughtful medical decision-making that used to be the ideal. And if you think things are bad now, they are likely to get much worse, as the population continues to get older, hospitals struggle with staffing and finance issues, and long-term care spots are expensive and in short supply.
Increasingly, patient care in the ER, once the patient makes it out of the crowded waiting room, is often a game of chance as to whether they can be quickly admitted. Gurneys often line the hallways, as beds are not available to admit patients assessed to need further testing or acute care. This logjam is called “Boarding.” That means patients who are assessed to need acute medical care cannot yet be taken to an inpatient bed, as there are none available. Therefore, patients may sit (or lie down) in the ER for hours or even more, without the kind of appropriate medical care they are assessed to need, and with the risk of further medical problems as they await their hospital inpatient bed. As one emergency department physician recently wrote, “ER boarding is a pervasive and worsening national crisis for hospitals. As more patients spend longer times in the ER waiting for an open hospital bed, the number of available beds for new patients dwindles.” The pile-up of patients in the emergency department is not only a byproduct of staff shortages and few inpatient hospital beds. Many adults, including older adults, simply cannot get access to a primary care physician in the community (don’t even think about access to a geriatrician), so they may delay seeking care until it reaches an emergency level. Others lack insurance to easily access care and go to the ER as a last resort. The care patients receive in the ER, however, may be suboptimal- not because the staff of the ER is incapable, but rather in the chaos of the ER hallway, it may be impossible to do a comprehensive physical exam or appropriate testing, if clothing can’t be removed, equipment can’t be accessed, or full medical histories cannot be obtained.
For older adults with cognitive impairment or dementia, the situation is even worse in the ER. The crowds, the noise, the lights, and the chaos of an ER can provoke distress in a person with dementia. This may not only trigger behavioral problems but may also lead to problematic outcomes for such patients and their families, including longer hospital stays, hospital readmissions, and even increased risk of death. As one concerned physician exclaimed, “Do not bring a patient with dementia to the emergency room unless she is turning blue.” While some hospitals have special emergency rooms for older adults (akin to having special places for pediatric patients), the reality is that small tweaks could make the general ER experience much better for patients with dementia, including allowing family caregivers to stay by the side of the patient, finding a quiet space for examinations, processing them quicker in the triage line and helping staff understand how to better communicate with such patients and their families. Unfortunately for older patients in the ER, every hour spent in the ER environment increases the risk of immobility or delirium for the patient. Especially for older patients already suffering from cognitive impairment or dementia, they are at significant risk for ER-acquired delirium, a state of confusion that can last well beyond the hospitalization. For more on ER-acquired delirium, click here.
So, how can you or a loved one limit the need to head to an ER (that is, unless you’re turning blue) or make the ER experience less challenging? You might first want to consider whether you or your loved one requires the level of testing and examination that an ER would entail. Obviously, if you have signs of serious distress, such as symptoms of a stroke or heart attack, heading to an ER and getting help as quickly as possible is imperative. Alternatively, if your symptoms are somewhat milder and perhaps less distressing- such as cold and flu symptoms, rashes, or mild trauma such as a scrape from a fall- you may want to turn to an Urgent Care Center in your local community, an alternative to seeing your primary care physician, who may be unable to give you a speedy appointment, or perhaps you have no primary care physician.
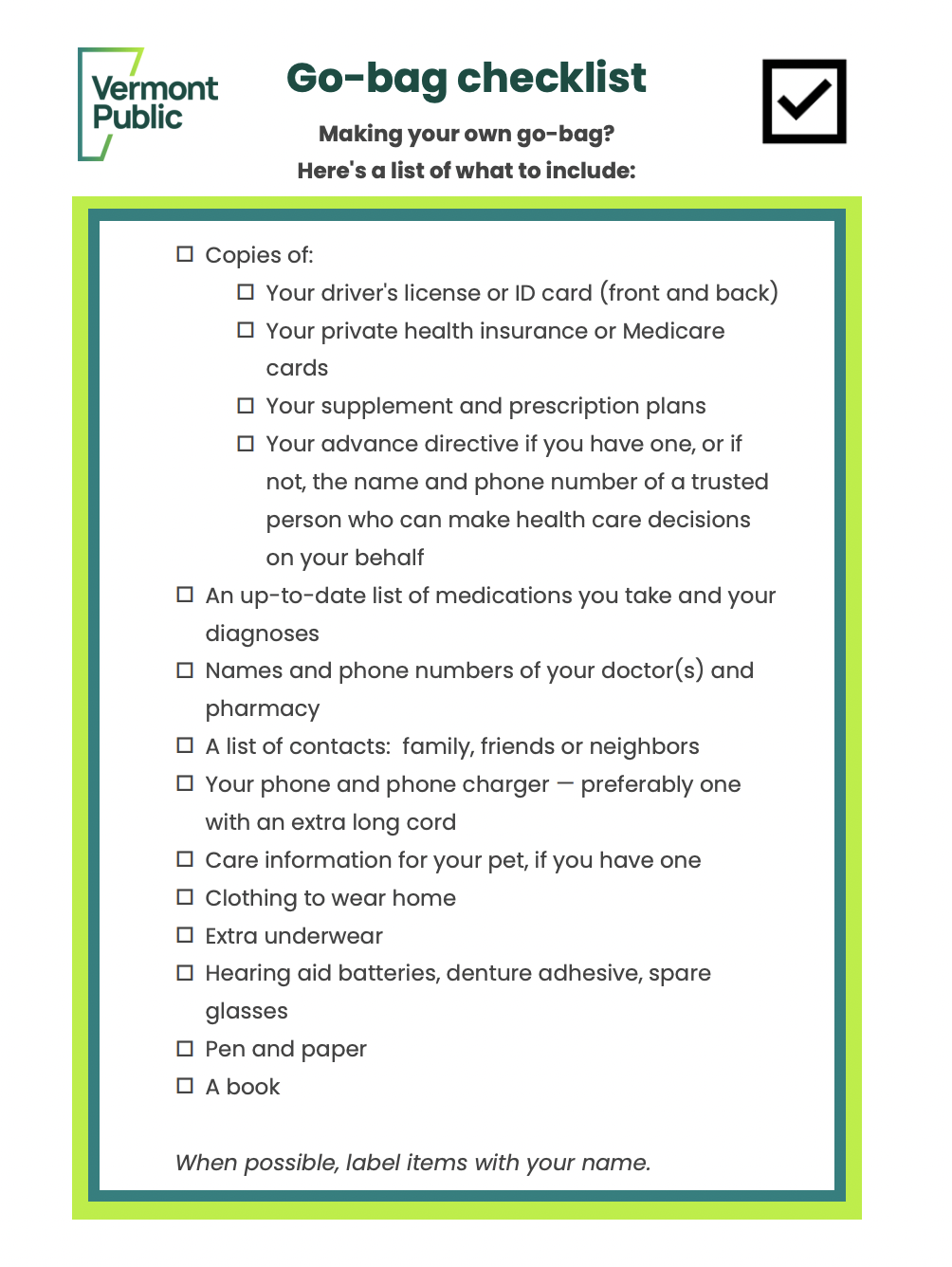
Another way to lessen the stress of a hospital ER visit is to be prepared in advance, so that questions about medical history, medications, and advance care directives are easily accessible to you, your loved ones, and hospital staff. Care.com recently published an emergency medical checklist to help you organize in advance of an emergency room visit. Alternatively, Vermont Public Radio has a checklist for not only the information you should have ready but also supplies you want to make sure you can grab and go. So find a spare backpack and take a look at their list here: